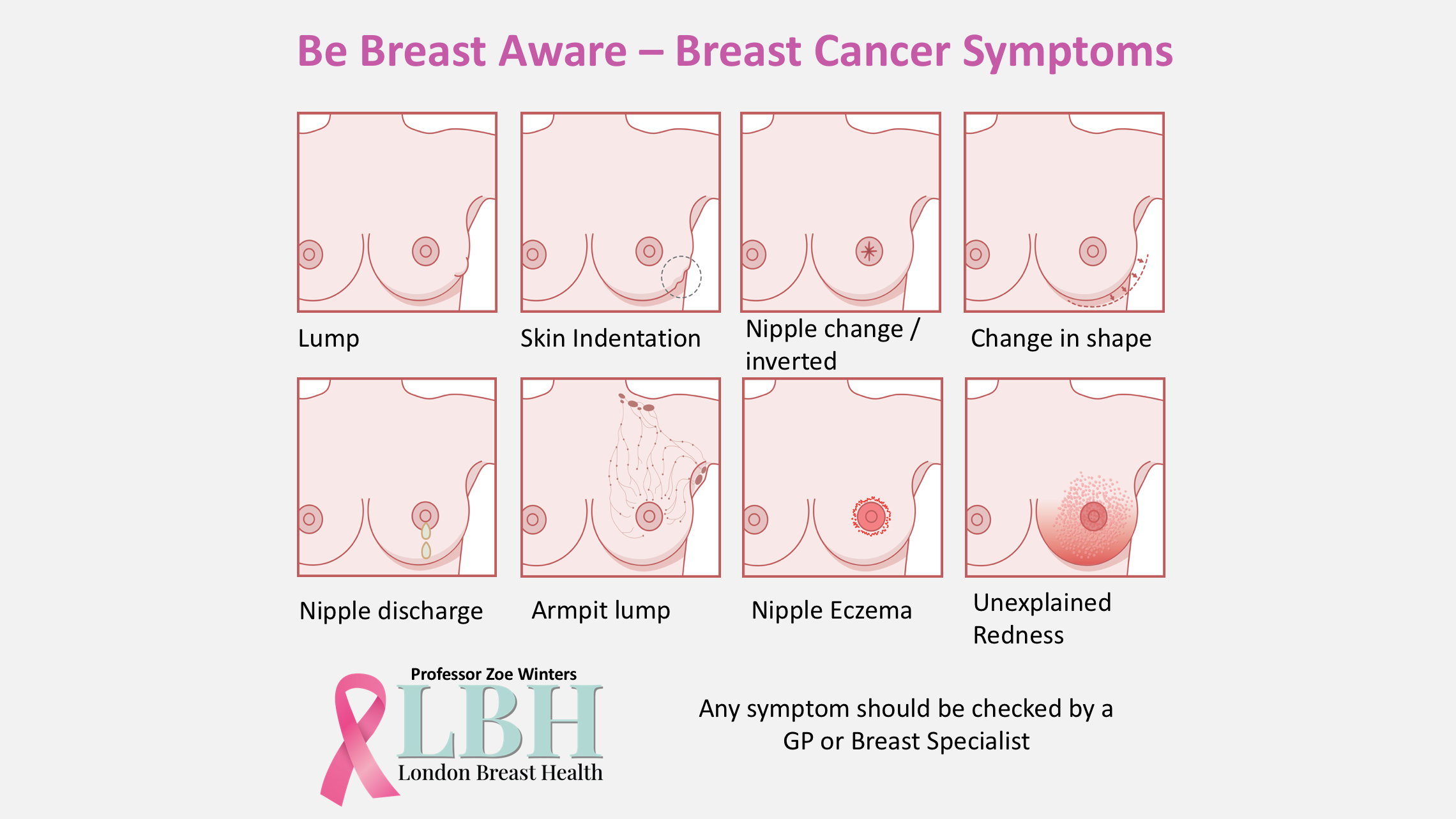
If you note the following signs please see your GP or Consultant Breast Specialist in the first instance.

LUMP
A breast lump is the most common symptom of breast cancer. On clinical examination, It is described as having a defined border, as though someone has placed a “marble” within the breast, which in principle means that one could get a pen and draw a border around it. If one is able to conceive this impression, then there is a high likelihood that you are feeling a true lump, that is clearly defined. This is quite distinct from a nodular firmness where breast duct tissue undulates under the skin and feels irregular, but is continuous over a large area, which is part of normal breast tissue.
Some people have firmer or more nodular feeling breasts based on one’s breast tissue density, or the amounts of firm breast ductal tissue compared to more fatty breasts, that feel softer. It is important to be breast aware, and to perform breast self examination.
Breast examination can be  performed in the shower using the flat of the hand as though one is feeling from the skin downwards, comparing this to pressing down onto a mattress, that varies in consistency. A firmer nodular breast feels like the “cobbles in a street”, and is mostly in the upper central and outer breast areas. The softer fatty breast areas are in the lower central breast where there is much less ductal tissue.
performed in the shower using the flat of the hand as though one is feeling from the skin downwards, comparing this to pressing down onto a mattress, that varies in consistency. A firmer nodular breast feels like the “cobbles in a street”, and is mostly in the upper central and outer breast areas. The softer fatty breast areas are in the lower central breast where there is much less ductal tissue.
A lump can be found in the breast, close to the armpit area, or in the armpit.
Most perceived lumps are not cancerous. Normal benign lumps may comprise a benign fibroadenoma, that often occurs in puberty and is a benign developmental lump. Breast cysts are common and relate to the sudden awareness of a new lump, that arises based on normal age-associated changes that occur in the breast ducts such as duct dilatation, with intraductal secretions that produce inflammation with debris that blocks microscopic ducts to produce a fluid filled cavity or cyst.
Other benign or normal lumps vary from a fatty lipoma (benign fatty lump with a border), injury related fat necrosis, a developmental hamartoma (encapsulated “breast within a breast”), a milk filled cyst or galactocele that occurs during pregnancy, or an infected cyst or abscess that is associated with inflammation.
All perceived lumps however, need to be clinically checked to rule out cancer.
NIPPLE CHANGE

Nipple changes that are indicative of a cancer:
Inverted or permanent indrawing of the nipple and/or the surrounding areola is clinically concerning. If this change is accentuated when one raises your arms, this increases concern.
A cancer produces an inflammatory reaction (part of one’s immune defence), that increases tissue scarring, and pulls in adjacent tissues with it, to permanently dimple or indent the nipple. This may be visible as a nipple depression or distortion of the breast.
Nipple Eczema must be differentiated from eczema of the areola.
Nipple Eczema that is  indicative of a cancer:
indicative of a cancer:
Eczema that starts on the nipple is concerning, and should be distinguished from eczema of the areola, where areolar eczema is part of a skin condition, and merits a referral to a Consultant Dermatologist.
Persistent and erosive eczema of the nipple only, of which the signs are itching, scaling, red or raised plaques and discharge from the nipple, may indicate Paget’s disease of the nipple. Paget’s disease of the nipple is rare, and usually occurs in older women. It may be isolated to the nipple, presenting as a clinical stage 0 breast cancer, or Ductal Carcinoma in Situ (DCIS).
Any nipple changes as described above, should be checked by a Doctor or a Consultant Breast Specialist.
NIPPLE DISCHARGE

Nipple Discharge that may be normal :
Normal nipple discharge can be intermittent, spontaneous, and straw coloured, with discharge that varies in its volume. Breast ducts open microscopically onto the skin of the nipple.
Breast ducts are channels that are lined by breast duct epithelial cells, and are responsive to hormonal stimulation by oestrogen, progesterone, and prolactin (milk producing hormone). Normal factors that raise these hormones are the: contraceptive pill, pregnancy, breast feeding, HRT, IVF, and antidepressants that (secondarily) raise prolactin levels. These factors can lead to normal or physiological nipple discharge.
Breast ducts age after pregnancy, and breastfeeding, with contributions by individual genetic factors. This results in breast duct wall thinning, with duct dilatation, leading to stagnation of secretions within ducts. These changes are called ductal ectasia or prominent ductal dilation, that can produce normal nipple discharge.
It is important that women are not alarmed by this change, but should still seek the expert advice at a One-Stop breast clinic.
Nipple Discharge that maybe abnormal:
Excess milky nipple discharge is called galactorrhea, and is defined as an increased volume and frequency of milky nipple discharge in the non-lactational breast. It is important to exclude commonly occurring contributors such as drug induced galactorrhea, that is secondary to antidepressants or selective serotonin uptake inhibitors (SSUIs), that increase serotonin in the brain, and also increase blood prolactin levels. A number of sedatives and antipsychotics may also produce this effect.
Excess breast stimulation is another factor that emulates the milk duct reflex (eg. similar to when the baby breast feeds), and produces increases in the milk producing hormone, called prolactin.
Other conditions of the pituitary gland called a benign adenoma (or growth), may produce significant increases in prolactin levels. A suspected prolactinoma is diagnosed on a CT scan or an MRI of the brain.
Excess milky nipple discharge in the non-breastfeeding breast should be assessed by a breast specialist in a one stop clinic

Nipple discharge bloody
(not breast milk) / (other than breast milk)
This presentation is clinically concerning and should always be reviewed by a breast specialist in a one stop triple assessment clinic. However, bloody nipple discharge is frequently benign. Often there is no clear lump or change on mammograms.
It is important to exclude abnormal breast cancer cells within a microscopic duct called ductal cancer in situ (DCIS). This may present with breast calcifications on the mammogram, or is challenging to see in the area directly behind the nipple, where abnormal cellular changes are often mammographically occult (not seen on imaging). Breast ultrasound of the ducts under the nipple is key in demonstrating a focal lesion that can be biopsied, such as a papilloma or polyp like lesion within a breast duct. Any focal area of abnormality will undergo an image guided biopsy.
The positive predictive value for detecting malignancy for an abnormality found on mammography was 53.5%, and for ultrasonography, it was 65.2%. The role of cytology (cellular analysis of the fluid) in detecting malignancy was inconclusive, and is generally unreliable.
Breast MRI is important to complement a mammogram and ultrasound findings, and is indicated before any surgical excision. Clinicians must endeavour to diagnose the cause of the bloody nipple discharge before any surgery intervention such as benign inflammatory changes may also produce a bloody nipple discharge secondary to secretions and inflammatory debris that collects within dilated ducts called ductal ectasia. MRI guided vacuum biopsy is important where there is a specific type of enhancement.
In some cases, the cause for galactorrhea may not be found, and is called idiopathic.
It is important to identify potential causes, and to measure blood prolactin levels, where high prolactin levels can be treated with a drug called Cabergoline.
Bloody nipple discharge is mostly benign, but requires triple assessment with examination, mammogram, ultrasound and breast MRI guided biopsy of any lesion.
BREAST SKIN INDENTATION

A cancer produces an immune response by the body that results in inflammation and causes a secondary fibrosis or tissue scarring. This scarring pulls in or distorts surrounding tissues. This can be subtle and may appear as a temporary skin indentation or shadow, when you compress the skin between two fingers, or elevate the arm.
In principle, one may miss this symptom, therefore if you think you can feel a lump, try and assess whether you think there may be a skin shadow or indentation, when performing the above steps.
Skin indentation remains an important sign even in the absence of a lump. You should always seek a Specialist Breast Cancer Consultant’s advice at a symptomatic One-Stop clinic, undergoing a thorough clinical examination and comprehensive breast imaging.
CHANGE IN SIZE  OR SHAPE
OR SHAPE
Swelling (increase in size)
The normal breast size changes with monthly fluctuations in oestrogen and progesterone, that relates to the menstrual cycle, called a premenstrual syndrome. Swelling and breast tissue tenderness may affect only one breast, as the right and left breasts are normally different in the way they develop when the foetus is in the womb, Therefore, there are normal developmental differences between one’s breasts such as size, shape, position of nipples, and in the amounts of breast ductal tissue and fat. One may have more breast duct tissue in one breast and therefore produce more milk from this breast compared to the other.
Normal breast swelling therefore fluctuates, and is called cyclical.
Abnormal breast swelling that is more concerning, is persistent and increases over months. This may also be accompanied by other persistent abnormalities such as skin changes, a nipple discharge, breast lump, or a swollen armpit (axillary) with lumps or enlarged lymph nodes.
Shrinkage (decrease in size) 
Abnormal breast shrinkage is persistent, and becomes more noticeable over time. This may also be accompanied by other persistent abnormalities such as skin and/or nipple changes, nipple discharge, breast lump, or a swollen armpit (axilla), with lumps or enlarged lymph nodes.
The feel of the breast tissue may feel firmer, with decreased elasticity when you depress the tissue. These changes are concerning as they reflect scarring (fibrosis) of breast tissue secondary to a diffuse or large cancer.
Persistent breast shrinkage is rare, and is usually associated with abnormal breast skin changes in keeping with aggressive cancers that are locally advanced.
A LUMP OR
 SWELLING IN EITHER OF YOUR ARMPITS
SWELLING IN EITHER OF YOUR ARMPITS
Swollen Nodes: Axilla (armpit) and above the clavicle (collar bone)
Lymph nodes are small, bean-shaped masses of lymphatic tissue, that receive lymph fluid from the lymph vessels. 75% of the breast lymphatics drain to the axillary (armpit) nodes, and to the internal mammary lymph nodes, within the chest wall alongside the breast bone (sternum).
Lymphatic circulation in breast tissue helps regulate the local fluid balance, and filter out harmful substances.The breast’s lymphatic system can also spread diseases such as cancer through the body.
Lymph contains fluid that escapes from body tissues, and contains white cells that fight infection, and foreign material like cancer cells.
Lymph nodes in the armpit can feel enlarged after any breast infection or following a breast tissue biopsy. Normal lymph nodes are assessed using ultrasound of the armpit. It is rare however, to feel lymph nodes above the collar bone.
Invasive breast cancers where cancer cells have invaded outside a microscopic breast duct can invade lymphatics, and drain via this circulatory system to the armpit lymph nodes.
Clinical examination and axillary ultrasounds are frequently performed as part of overall breast assessment in a one stop clinic.
UNEXPLAINED
 REDNESS
REDNESS
A rash or itchiness, a scaly appearance, unusual redness or other colour changes
Inflammatory breast cancer develops when cancer cells invade the skin lymphatics and block lymph vessels. Lymph vessels are hollow tubes that comprise your lymphatic system, that normally allows lymph fluid to drain out of your breast tissues. Cancer cells blocking the lymphatic vessels cause your breast skin to appear pink, reddish purple, or bruised.
Blocked skin lymphatics cause lymphoedema or thickening of the skin, causing the typical orange peel appearance called “eau d’orange” (pitted skin appearance of an orange peel). These features are indicative of locally advanced invasive breast cancer, and inflammatory breast cancer (IBC).
IBC is a rare type of breast cancer that comprises only 1% to 5% of all breast cancers. It often doesn’t cause a lump, or show up on a mammogram, so it can be difficult to diagnose.
Other symptoms of IBC include:
- Pain (differs from breast pain syndrome that shows no other symptoms)
- Swollen lymph nodes (see swollen nodes)
- Firm or hard breast that is hot to the touch (see lymphoedema)
- Changes to the nipple such as flattening or an inverted nipple (see nipple changes)
- A rapid increase in the size of a breast (see changes in breast size, shape)
_____________________________________________________________________________________________
Be breast aware. Learn what your breasts look and feel like. Get to know what is normal for you. The appearance and feel of breasts can change at different times of the menstrual cycle. The milk-producing tissue in the breast becomes active in the days before a period starts. In some women, the breasts at this time feel tender and lumpy, especially in the upper-outer part of the breast near the armpits.
After a hysterectomy (removal of the womb), the breasts usually show the same monthly changes until the time when your periods would have stopped naturally.
After the menopause, activity in the milk-producing tissue stops. Normal breasts can feel soft, less firm and not lumpy.
Check your breasts monthly. Any changes, see your GP or make an APPOINTNMENT HERE